Abstract
Contemporary models of perception characterise the brain not as a passive receiver of sensory input but as a predictive system that actively constructs experience from the top down. This paper brings together predictive processing accounts of interoception and selfhood, enactive and phenomenological accounts of embodiment, and the Ten Fetters (samyojana) of the Buddhist Pali Canon, a 2,500-year-old taxonomy arrived at through an entirely different method, to ask whether they are independently describing the same structure.
We propose they are: that a significant class of human suffering is better understood as the self-model becoming too rigid to update, rather than as a problem with specific thoughts, memories, or symptoms. The purpose of this paper is to specify that mechanism precisely enough to be tested, not to demonstrate that it explains suffering.
We report exploratory pilot data (n=19) from the Odoki Method, a structured somatic inquiry intervention designed to interrupt this proposed mechanism directly, without requiring participants to understand the theory behind it. Pre/post psychometric data show shifts consistent with the account, and motivate the mechanistic and controlled studies proposed in the conclusion. The data illustrate the theoretical claim; they do not establish it.
Theoretical Background & Literature Review
1. The Predictive Brain and Simulated Reality
Predictive Processing and Core Affect (Lisa Feldman Barrett)
Barrett’s theory of constructed emotion proposes that the brain functions as a predictive system rather than a passive receiver of sensory input (Barrett, 2017). Rather than reacting to the world, the brain continuously generates and updates an internal model of the body-in-the-world, anticipating sensory input on the basis of prior experience.
Two features of this account are particularly relevant here.
First, the brain’s primary regulatory task is allostasis: keeping the body in balance. To do this, it monitors internal bodily signals (interoception) and generates a continuously updated, pre-verbal summary of physiological state, which Barrett terms core affect. It is the brain’s ongoing, pre-verbal assessment of the body’s metabolic condition.
When incoming interoceptive signals deviate from the brain’s predictions, the resulting mismatch - a prediction error - is not discarded. Instead, it drives a response: the brain either revises its predictive model to better match what it is receiving, or takes allostatic action on the body itself to bring it back in line with its predictions. Core affect, on this account, is less a passive readout of current bodily state than a running summary of this ongoing effort to keep predictions and reality aligned.
Second, the brain deploys learned conceptual categories to interpret this raw affective signal. An accelerated heart rate may be categorised as fear in one context and excitement in another. Without such top-down conceptual scaffolding, internal and external sensory experience would, as William James observed, remain a blooming, buzzing confusion. The categories that the brain applies are not neutral; they are shaped by prior experience, language, and culture.
This interoceptive dimension is clinically significant: disruption to the sensation, interpretation, and prediction of bodily signals is reliably observed across a wide range of mental health conditions, suggesting that interoception may function as a transdiagnostic mechanism - a common factor underlying many mental health conditions - across diverse forms of psychological distress (Hickman et al., 2025).
Predictive Accounts of Selfhood (Anil Seth)
Seth and colleagues extend the predictive processing framework to the experience of selfhood (Seth & Tsakiris, 2018; Seth, 2013). On this account, the sense of being a unified self - persisting through time, bounded by the body, the subject of experience - is itself a top-down predictive construction rather than a direct readout of reality. Sensory data does not create experience, it corrects it, keeping the brain’s predictions tethered to physical reality. Seth terms this everyday perceptual experience a “controlled hallucination”: controlled because the predictions are continuously tested against sensory feedback, hallucinatory because the resulting experience is a brain-generated model rather than unmediated contact with the world (Seth & Tsakiris, 2018).
Crucially, this account extends to the observer. The felt sense of a stable, continuous self is, on this view, another layer of prediction - one with deep evolutionary roots in the need to maintain a coherent agent in the world, but no less constructed for that.
The term self-model is drawn from Thomas Metzinger’s Self-Model Theory of Subjectivity, which argues that the phenomenal self is a representational construct rather than a substantial entity, and that the system generating this model typically cannot recognise it as a model - a property Metzinger terms transparency (Metzinger, T. 2003"). This transparency is directly relevant to the account developed here: it is precisely because the self-model is not experienced as a model that it becomes available for reification rather than revision.
In hierarchical predictive processing accounts, higher-level predictions that are held with strong confidence and updated only slowly are termed hyperpriors. The self-model, on this account, is among the most deeply weighted of these — a hyperprior that organises and constrains the interpretation of almost all incoming experience.
2. Embodiment and the Lived Experience
Enactive Embodiment (Evan Thompson)
Thompson argues that cognition is not the passive representation of an independently existing world but a process of sense-making (Thompson, 2007). A living system does not merely process information; it actively brings forth a world through its organised, metabolic activity. Mind and life are continuous rather than separate.
Central to this account is the distinction between the body as studied from outside and the body as experienced from within. Any meaningful shift in how a person experiences themselves is, on this view, not merely a cognitive event but a change in the biological and experiential state of the whole organism.
The Felt Sense (Eugene Gendlin)
Gendlin provides a precise phenomenological description of how the body carries meaning that has not yet been articulated in language (Gendlin, 1978; Gendlin, 1997). He terms this the “felt sense”: a holistic, meaningful, but initially unformulated bodily awareness of a situation or problem. A felt sense is not a discrete named emotion, nor a simple physical sensation. It is a complex, implicit knowing - a bodily awareness that exceeds whatever labels the mind has so far applied to it.
Gendlin’s account provides an experiential complement to Barrett’s interoceptive constructs: where Barrett describes the computational architecture by which the brain generates affective summaries, Gendlin describes what it is like, from the inside, to attend to that somatic signal before it has been conceptually packaged.
3. Phenomenological Psychopathology: The Shift to Suffering
Phenomenological psychopathology examines psychological distress as a disturbance in the structure of lived experience - in how a person experiences time, space, and selfhood - rather than as a collection of symptoms to be catalogued (Stanghellini et al., 2019). Two concepts from this tradition are particularly relevant to the present account.
The first is the pre-reflective sense of being a self (ipseity): the minimal sense of I-ness that anchors experience, making thoughts and perceptions feel immediately one’s own. In severe psychopathology this structure can become radically destabilised, as in early psychosis, where the sense of being a distinct self begins to dissolve.
The second is hyperreflexivity, a concept developed particularly by Sass and Parnas to describe an exaggerated, self-observing inward gaze that arises when pre-reflective experience is disrupted (Sass & Parnas, 2003). When the natural flow of experience breaks down, the mind turns an intellectualising attention on itself in an attempt to restore coherence. In its most extreme form this process can crystallise into delusional frameworks.
4. Contemplative Neuroscience and the Relaxation of Priors
A growing body of work in contemplative neuroscience has used the predictive processing framework to model the computational mechanics of deconstructive meditation practice (Laukkonen & Slagter, 2021). Extending this, Laukkonen, Friston, and Chandaria propose that the active inference loop is not merely the mechanism by which experience is generated but is constitutive of consciousness itself (Laukkonen et al., 2025).
Within a hierarchical predictive system, the brain’s most deeply learned patterns of thought are maintained with strong confidence - the brain treats its most entrenched expectations as highly reliable, and filters incoming data accordingly. Laukkonen and Slagter propose that deconstructive practices operate by systematically loosening this confidence: by directing attention away from conceptual content and toward bodily sensation, the brain’s grip on its most entrenched patterns begins to relax.
5. The Pali Canon: An Ancient Diagnostic Taxonomy
The Ten Fetters (samyojana) appear throughout the Pali Canon (Bodhi, 2012) as a systematic account of the cognitive and affective structures that bind the organism to suffering. For the canonical enumeration, see the Saṁyojanasutta (AN 10.13; Bodhi, 2012). Rather than approaching them through a religious or spiritual salvation lens, we treat them here as a historically precedented psychological taxonomy: a map of the cognitive-linguistic structures through which a dynamic organism constructs and maintains the experience of a fixed, separate self.
Read in alignment with the predictive processing account above, the Ten Fetters describe a layered architecture of this construction, from its deepest pre-reflective allostatic roots through to its most elaborated conceptual and linguistic forms. This structural alignment is developed in detail in Section 6.
6. The Odoki Framework: Systemic Theory and Deadlock
The Allostatic-Linguistic Loop
When we bring Barrett and Seth together with Thompson and Gendlin, a coherent picture of how psychological suffering becomes self-sustaining begins to emerge.
The brain’s primary directive is allostasis - the ongoing management of the body’s metabolic resources. To discharge this function, it continuously generates a subconscious predictive summary of the body’s internal state, experienced as a baseline affective tone. This is the organism’s somatic answer to a persistent implicit question: am I safe?
When the answer is no, the system registers a state of metabolic alarm. But the brain cannot tolerate an unresolved threat signal. It immediately deploys a second layer of prediction - linguistic and conceptual categorisation - in an attempt to identify and manage the source of danger. The vague somatic contraction of unsafety is assigned a label: I am anxious, I don’t like confrontation, people with this attitude should be avoided. In more extreme cases it can become: I am fundamentally broken, everything goes wrong for me, I cannot cope. The brain reaches for the most available label and applies it.
The difficulty is that this categorical move, designed to resolve the alarm, tends instead to entrench it. The organism stops experiencing a shifting, temporary biological state and starts experiencing a permanent identity. The metabolic signal becomes a self-description.
How the Loop Locks
This allows us to describe suffering with some structural precision. The problem is not the presence of an unsafety signal - that is a normal feature of biological life. The problem is the rigidity that follows from its conceptual capture.
When the brain categorises a somatic contraction as a permanent identity trait, it initiates a self-reinforcing loop:
- The brain predicts threat, generating an interoceptive summary of unsafety.
- It applies rigid top-down linguistic concepts, eventually interpreting the unsafety as evidence of a fixed, vulnerable self.
- That self must now be defended, which consumes metabolic resources.
- This metabolic cost generates a fresh interoceptive signal of unsafety, reinforcing the original prediction.
We term the consequence of this process the reification of the self-model: the gradual hardening of what is in fact a fluid, dynamic biological state into a felt, fixed identity structure. In individuals with maintained daily functioning, this loop rarely produces the reality-shattering disruption characteristic of psychosis. What it produces instead is a chronic, low-grade but pervasive sense of being trapped - unable to change the conceptual narrative because the allostatic system is signalling danger, and unable to resolve the allostatic signal because the conceptual narrative keeps the alarm active.
The Traditional Parallel
The Ten Fetters of the Pali Canon, read through the predictive processing framework developed above, describe this same architecture with notable structural precision.
The deepest layers of the taxonomy - avijjā and māna (the tenth and ninth fetters: ignorance and conceit) - describe the root of the construction. Avijjā is the fundamental error through which fluid experience is mistaken for fixed, self-existing things - the point at which concepts begin to be reified. Māna is where those reified concepts are turned outward: the self that has been solidified now asserts how the world ought to be.
The more accessible layers of the taxonomy, moving toward sakkāya-diṭṭhi (the first fetter, identity-view), represent the progressively more elaborated conceptual and linguistic structures built on top of that somatic foundation. These are the top-down models that rush in to label, explain, and rationalise the underlying allostatic signal - and that, in doing so, lock it in place.
That this structural relationship has been independently described across radically different frameworks and historical periods suggests it reflects something real about the architecture of human suffering.
The Deadlock
This points to a problem: if the brain is a predictive system that uses its existing high-level priors to interpret all incoming data, and if those priors have become organised around the defence of a reified self-model, then any attempt at self-correction faces a structural obstacle: the very apparatus being used to address the problem is the problem. Cognitive effort, philosophical reflection, and intellectual insight all operate within the same predictive hierarchy that maintains the loop. They cannot easily generate the kind of genuine prediction error that would be required to loosen its most deeply weighted priors.
This provides a specification of what an effective intervention would need to do: introduce a disruption that originates outside the individual’s existing predictive hierarchy, operates at the level of somatic attention rather than conceptual content, and provides sufficient safety for the system to tolerate the resulting uncertainty without immediately re-closing around a defensive prior.
The Odoki Method addresses this through a structured ten-stage sequence. The first two stages are preparatory, establishing the somatic attention required for the work that follows. Stages three through ten each target a discrete hyperprior layer in order of increasing subtlety, with each stage reducing the somatic noise contributed by its target and making the next stage’s target perceptible. The sequence appears to require this ordering; reordering it appears to disrupt the mechanism.
Relational Interoception
An Odoki Guide is a trained practitioner who takes a client through this structured sequence of somatic exercises. The exercises are conducted within a sustained relational container: the guide attends to the client’s present-moment bodily state in real time, making the interoceptive process a shared rather than a solitary one. This is what we term relational interoception - and its relational dimension is not incidental to the method but structurally necessary.
The guide is not primarily a source of emotional support, though the relationship carries that quality. Because the guide is a separate person, their attention is not subject to the client’s own prediction minimisation mechanism. This allows them to introduce a genuine corrective signal into the client’s predictive environment - one that the client cannot generate alone, precisely because their own apparatus for self-correction is entangled in the loop.
This account is consistent with Active Inference models of the therapeutic alliance, which propose that an attuned relational partner functions as a reliable presence that signals safety - allowing the individual’s system to loosen its defensive patterns without experiencing this as threat (McParlin et al., 2022). The guide’s sustained, non-reactive presence signals to the client that the immediate environment is secure enough to permit loosening of the conceptual armour without catastrophic consequence.
The guide also serves a second, more specific function: attentional governance. Left alone, a participant will typically find their mind jumping back to familiar labels before the bodily sensation has been fully registered. The guide interrupts this by holding attention on the somatic signal through precise, targeted prompts, preventing habitual patterns from reasserting themselves too soon.
The Odoki Method introduces a third structural feature, which we term the narrative exclusion rule: the guide does not learn, and actively avoids learning, the participant’s personal history or situational context, working solely with the present-moment somatic signal. Content-free approaches exist in somatic trauma therapies, typically to protect the participant from re-traumatisation, but the rationale here is different. The narrative exclusion rule serves a specific neuro-computational purpose directed at the guide rather than the participant: if the guide learns the narrative backstory, their own predictive engine begins modelling the participant’s situation, introducing top-down simulations that compromise their capacity to attend cleanly to the participant’s real-time somatic state. Remaining blind to narrative content keeps the guide’s attention anchored in the present somatic signal rather than in a conceptual reconstruction of the participant’s history.
Methodology
Study Design and Context
This paper presents findings from an exploratory pilot study of the Odoki Method, conducted as an iterative development protocol. The primary aims were to refine the delivery of the method through successive cohorts and to track psychometric change in participants using validated instruments. No control condition was included at this stage. The study is presented as preliminary evidence warranting more rigorous investigation, not as a demonstration of efficacy.
Participants
A convenience sample of 19 participants (n=19) was recruited through the extended networks of the project principals. No formal clinical prescreening was implemented. The cohort consisted primarily of individuals with maintained daily functioning experiencing chronic stress, burnout, or situational anxiety, alongside a small subset presenting with more severe subjective distress causing significant functional impairment. The recruitment method and sample composition impose clear limits on the generalisability of the findings, which are discussed in the conclusion.
Technical Infrastructure
All study activity was managed through a purpose-built web application, the Odoki Hub. This platform handled session scheduling, hosted the booking interface for video consultations, and served as the data collection portal for psychometric instruments. A Python data pipeline within the Hub enabled real-time data management and automated generation of visualisations. Video consultations were conducted via Google Meet.
Operational Parameters
Sessions were 30 minutes in duration and scheduled approximately weekly, though final frequency was determined by participant preference. The total number of sessions was not fixed in advance; progression was determined by the participant’s movement through distinct experiential stages. In earlier cohorts this required up to 20 sessions. As the lead guide’s practice developed and the method became more precisely operationalised, this reduced to as few as 10 sessions (approximately 5 hours of total contact time) in later cohorts.
Data Collection and Psychometric Instruments
Psychometric data were collected at baseline and at completion of the intervention using three validated instruments, administered digitally through the Odoki Hub:
- Quick Inventory of Depressive Symptomatology (QIDS-SR): Tracking shifts in depressive symptom severity.
- Generalised Anxiety Disorder Assessment (GAD-7): Measuring changes in anxiety levels.
- Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Monitoring holistic shifts in psychological wellbeing and functioning.
Data Analysis
Given the exploratory nature and small sample size of this study, inferential statistical analysis was not conducted. Two graphical outputs were generated to illustrate individual and cohort-level trajectories:
- Dumbbell plots (Matplotlib): Mapping pre- to post-intervention score changes for each participant across all three instruments.
- Sankey diagrams (Chart.js): Tracking cohort-level movement between severity categories across the course of the intervention.
Quantitative Analysis
1. Mental Wellbeing (WEMWBS)
The most consistent trend across the cohort occurred on the Warwick-Edinburgh Mental Well-being Scale. 18 of 19 participants reported a positive increase in their scores. The cohort mean rose from 34.1 at baseline to 49.3 at completion, a mean improvement of 15.2 points (Cohen’s d = 1.24, large effect). Using the WEMWBS minimum clinically important difference (MCID) threshold of 3 points, 18 of 19 participants (94.7%) achieved clinically meaningful improvement.
The single participant who did not show an increase (A007) recorded a reduction of one point (27 to 26). This participant withdrew from the protocol before completion to pursue alternative modalities; their post-intervention score therefore reflects an incomplete intervention rather than a completed one.
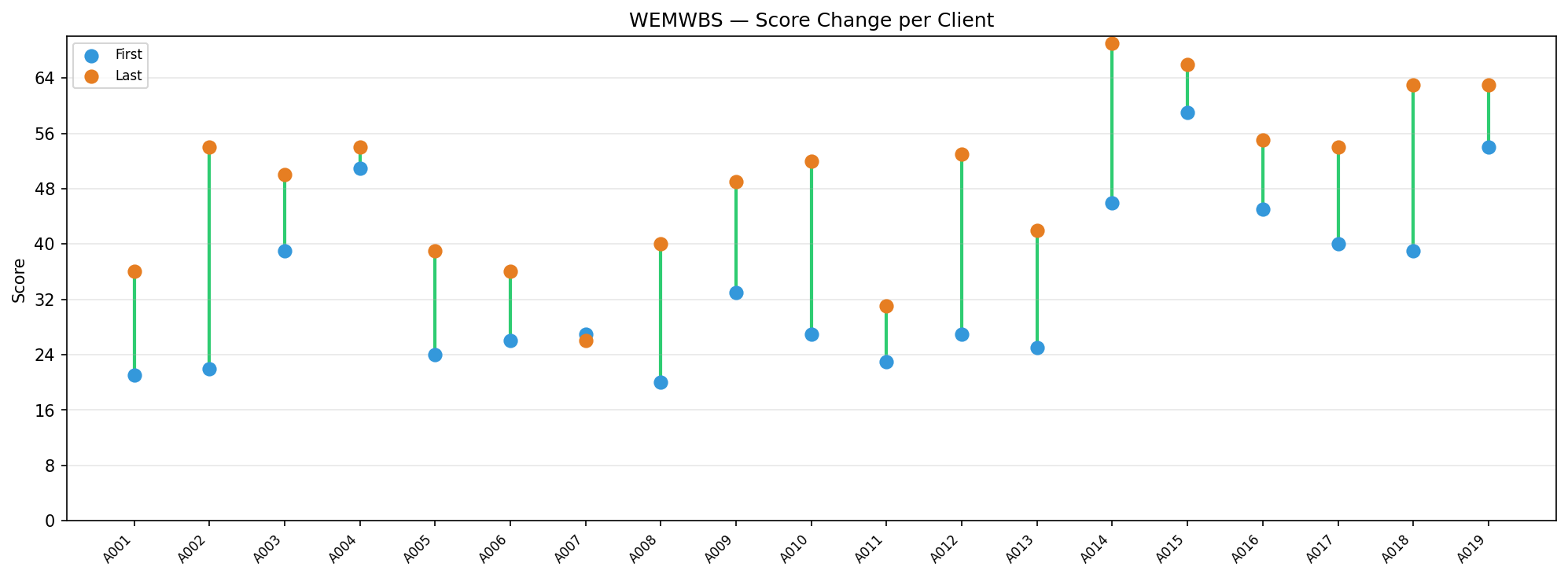
Figure 1: Pre- and post-intervention WEMWBS scores by participant.
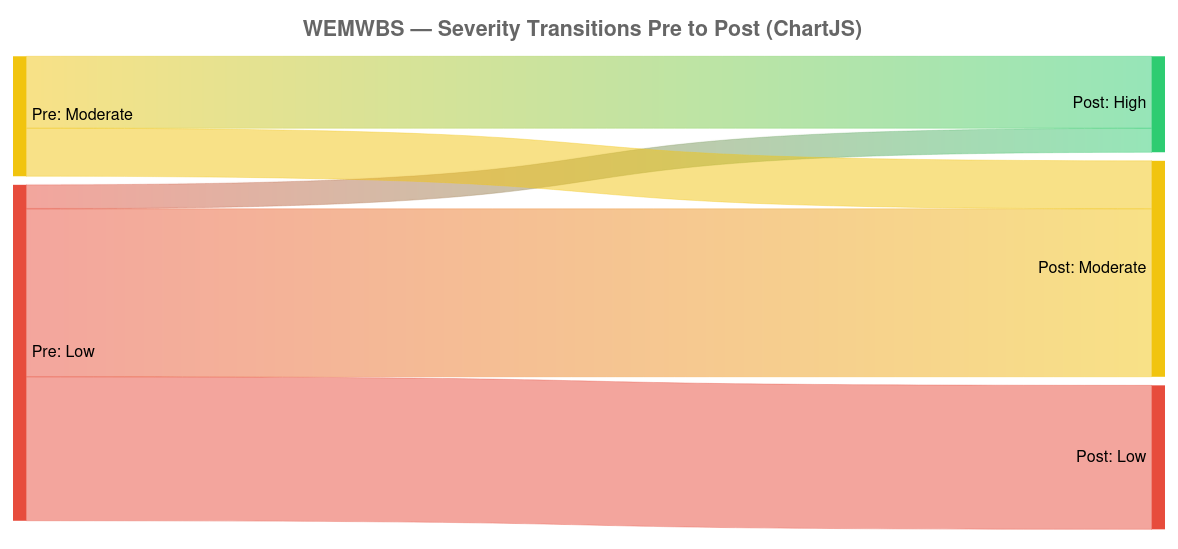
Figure 2: Cohort movement between WEMWBS severity categories.
2. Depressive Symptomatology (QIDS-SR)
The cohort mean fell from 6.6 at baseline to 3.5 at completion, a mean improvement of 3.1 points (Cohen’s d = 0.91, large effect). 16 of 19 participants showed some reduction in scores. Using the QIDS-SR MCID threshold of 5 points, 7 of 19 participants (36.8%) achieved clinically meaningful improvement.
The majority of the cohort presented with mild or minimal baseline scores, which both limits the scope for MCID-level change and reduces the strength of conclusions that can be drawn about the method’s performance with more severely depressed populations. Within the cohort, however, the categorical shifts for higher-baseline participants were notable: the moderate depression bracket was entirely evacuated by the end of the intervention, with one participant moving from moderate to mild and another moving from moderate to the minimal range.
Of the three participants who did not show any reduction, one remained unchanged and two showed a one-point increase, both at the floor of the scale. These fluctuations are not considered clinically meaningful.
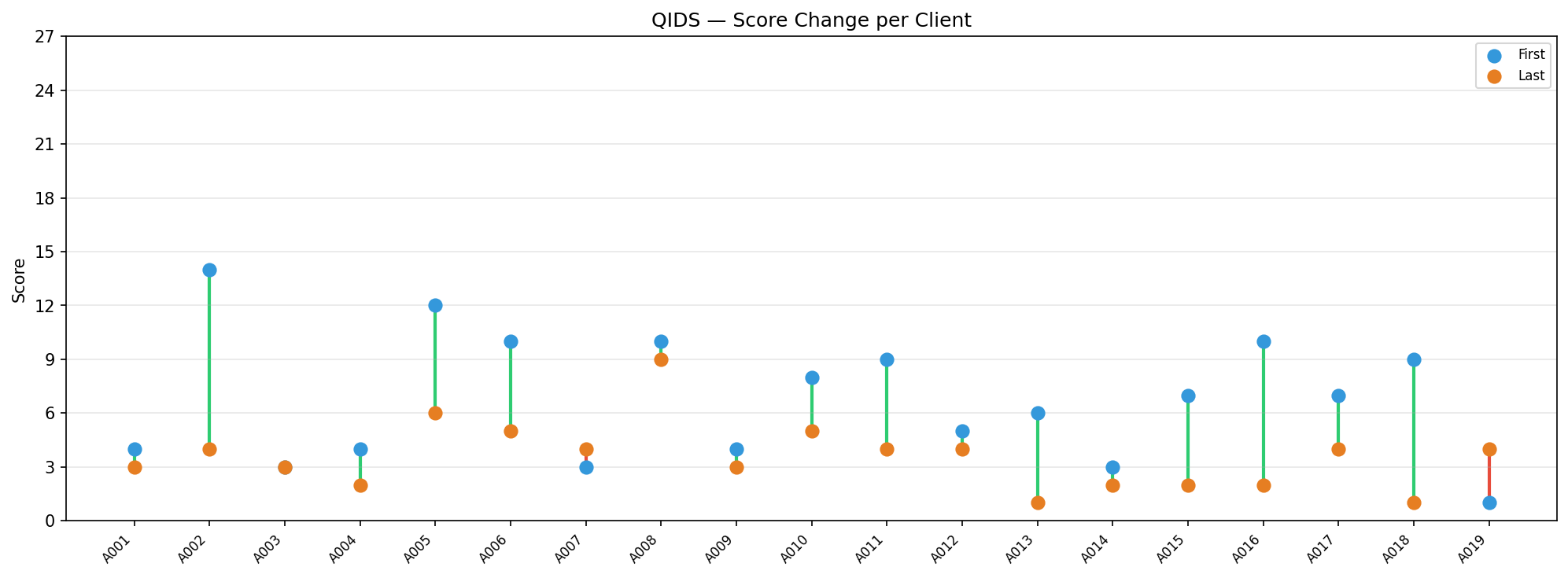
Figure 3: Pre- and post-intervention QIDS-SR scores by participant.
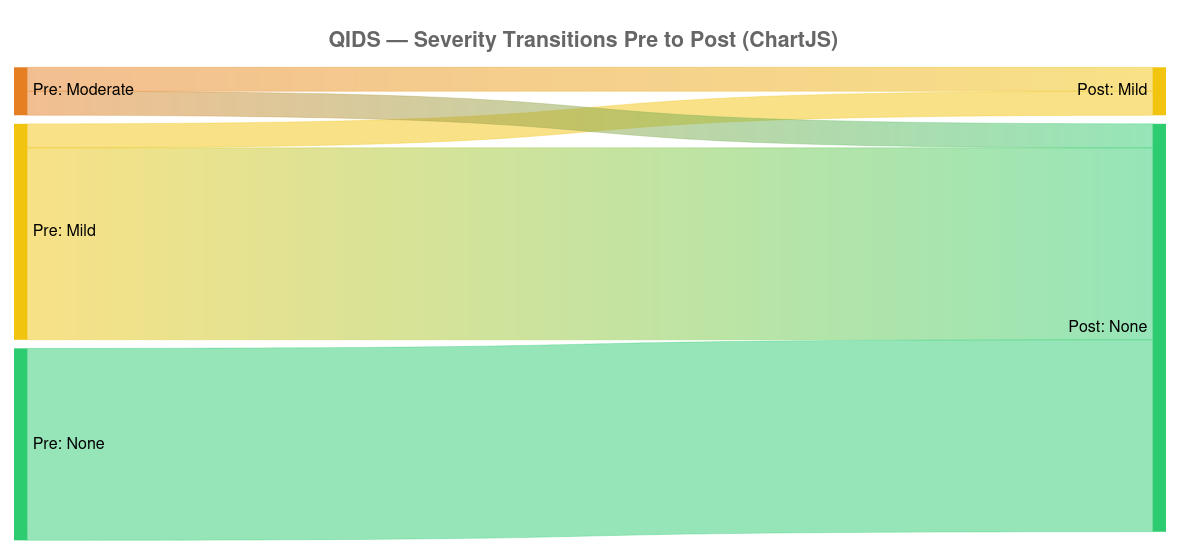
Figure 4: Cohort movement between QIDS-SR severity categories.
3. Generalised Anxiety (GAD-7)
The cohort began with a mean GAD-7 score of 10.8 (moderate anxiety bracket) and ended at 7.1 (mild anxiety bracket), a mean improvement of 3.7 points (Cohen’s d = 0.76, medium effect). 14 of 19 participants showed some reduction in scores. Using the GAD-7 MCID threshold of 5 points, 8 of 19 participants (42.1%) achieved clinically meaningful improvement.
The five participants who did not show improvement (A003, A006, A009, A012, A015) warrant specific consideration, and two hypotheses are offered for future investigation.
The first is a transitional arousal hypothesis. A system that has been functioning in a hypo-aroused, depressive state may need to pass through a period of increased activation before it can fully regulate. An upward movement on the GAD-7 during this transition may reflect nervous system activation rather than worsening anxiety in any stable sense.
The second concerns the limited vocabulary of the GAD-7 itself. The method works directly with somatic states that participants have previously labelled as anxiety. As the top-down conceptual structures that generate those labels begin to loosen, participants may encounter raw autonomic activation that they continue to code as anxiety on a self-report instrument, even when the underlying somatic shift represents movement toward greater flexibility rather than away from it. The word anxiety may be too coarse an instrument to track what is actually changing. This is a hypothesis, not a finding, and would require more granular phenomenological data to evaluate.
It is relevant to note that for all five participants who did not show improvement on the GAD-7, wellbeing (WEMWBS) improved without exception, and four of the five also showed improvement or no change in depressive symptomatology (QIDS-SR). No participant showed deterioration across all three measures. In the case of A003, the baseline GAD-7 score of 1 renders a one-point rise clinically uninterpretable. This cross-instrument pattern is inconsistent with a straightforward worsening of condition in any of the five cases, and lends substantive support to the transitional arousal hypothesis: what the GAD-7 is registering may be activation rather than deterioration. A more granular phenomenological account of these participants’ experience during and after the intervention would be required to evaluate this further.
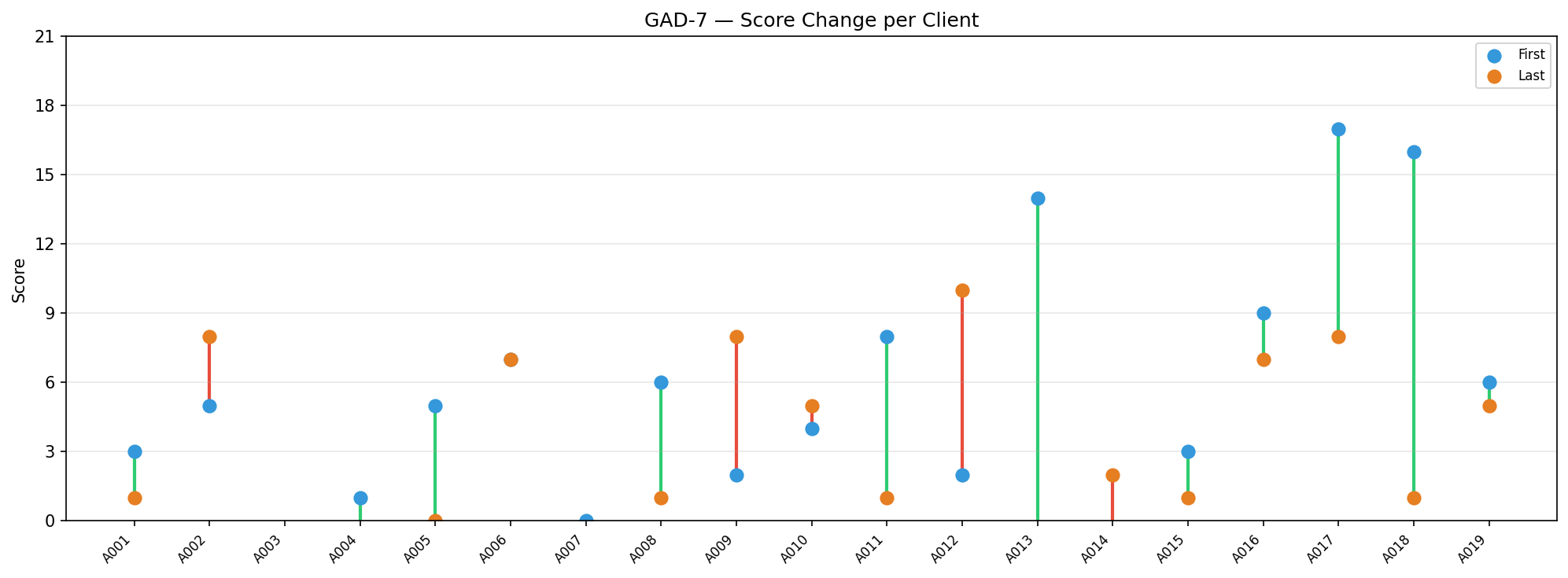
Figure 5: Pre- and post-intervention GAD-7 scores by participant.
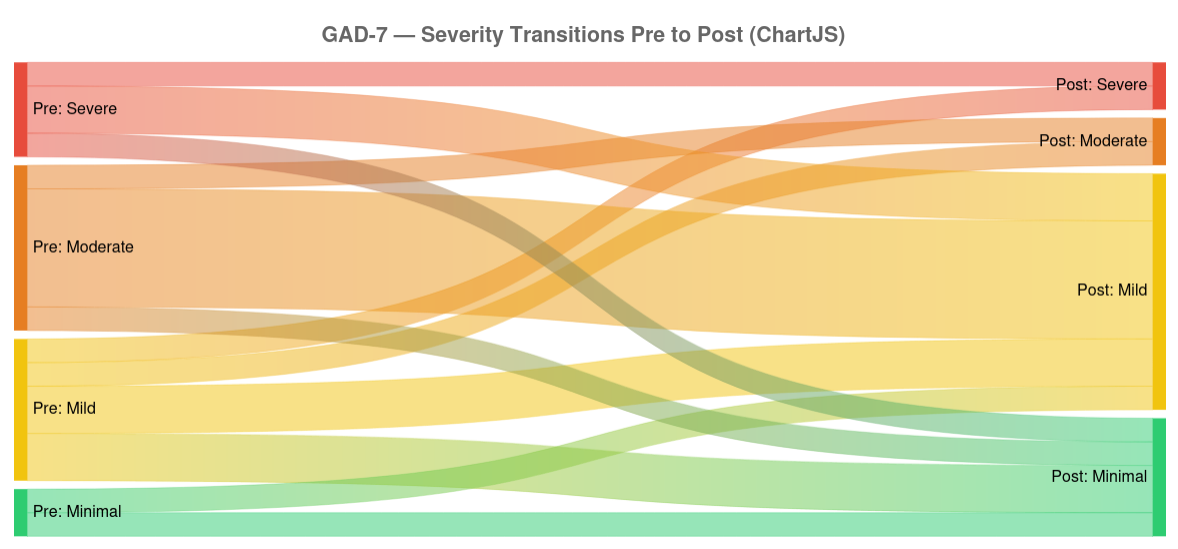
Figure 6: Cohort movement between GAD-7 severity categories.
Qualitative Analysis
The qualitative feedback collected through the Odoki Hub contextualises the quantitative trajectories described above. Three themes are presented here, drawn from participant responses at completion of the intervention.
Bypassing Narrative Constraints
The velocity observed in later cohorts - participants completing the full process in as few as ten sessions - is consistent with participant accounts of what made the method distinctive. Several participants with prior therapeutic experience commented specifically on the absence of narrative content as a differentiating feature:
“I have been doing therapy since I was a child, and it was the first time I didn’t have to talk about personal stories, issues etc. I think Odoki is a great option for people who find it difficult to open up. It is a very unique approach, challenging traditional talking therapy - a way, in a very short amount of time, to reconnect with how you feel in the world and how you react to triggering situations.”
By not asking participants to share their personal history, the method significantly lowers the barrier to trust. There is nothing to disclose, no story to be judged, and no vulnerability required beyond attending to what is already present in the body. The relational foundation forms more quickly as a result.
Shifts in Perceptual Experience
The large WEMWBS shifts observed in the quantitative data are reflected in participant accounts that describe changes not in symptom levels but in the quality of experience more broadly:
“I would say that Odoki has given me a completely new way of understanding the world and the way I perceived it. It allowed me to calm my anxious mind, to pause and reflect in my day to day. It has opened up for me a new way of understanding and listening to my body.”
This framing - a change in how the world is experienced rather than a reduction in specific symptoms - is consistent with the theoretical account offered in Section 6. If the intervention is operating at the level of the self-model rather than at the level of symptomatic content, participant experience of its effects would be expected to have this character.
Between-Session Support: The Kiri Chatbot
A third theme mentioned by clients concerns the role of between-session continuity. The Odoki Hub includes a prototype AI chatbot, Kiri, designed not merely as a support tool but as an implementation of the guide function itself. Kiri operates from the same protocol used to train human guides, and in its current form is capable of moving between stages of the method and requesting appropriate exercises for each stage - replicating, in principle, the attentional governance function of a human guide.
Several participants within this cohort described earlier versions of Kiri as enabling meaningful engagement with the process outside of formal sessions:
“The insights build upon each other in a way which makes them feel very solid. The Kiri chatbot was invaluable in enabling me to do the exercises in between sessions, which makes a big difference to progress. It also means that you’re not reliant on having sessions to do the work - you can do it any time when you need it.”
Among users outside of this study cohort, approximately four people have engaged with the current iteration in a way that meaningfully replicated the guide dynamic. The primary limitation identified is in the early stages of interaction. Before the method proper can begin, a guide must establish sufficient relational trust that the participant is willing to follow their direction. Without this foundation, the subsequent process cannot take hold. Human guides build this responsively, reading and adapting to subtle signals that indicate whether that trust has been established. We have not yet tested the extent to which the current prototype can reliably detect when the relational foundation is in place before proceeding.
Kiri is mentioned here for completeness; its development falls outside the scope of this study. The trust problem is nevertheless worth noting, as the reason matters. The guide’s function as a reliable, trusted presence that signals safety - as described in Section 6 - is not simply a matter of delivering the correct prompts in the correct sequence. It depends on the participant having first experienced the guide as trustworthy enough to lower their defences. Replicating that relational quality algorithmically is a non-trivial problem, and one with significant implications for the scalability of automated delivery.
Conclusion and Future Horizons
The results of this exploratory pilot study suggest to us that the Odoki Method warrants more rigorous investigation. The findings - consistent improvements in wellbeing, meaningful reductions in depressive symptomatology, and partial reductions in anxiety across a small convenience sample - are not sufficient to establish efficacy. What they do establish is a pattern of change consistent with the theoretical account offered in this paper, and a preliminary evidence base sufficient to motivate a controlled mechanistic study.
The Narrative Exclusion Rule as a Theoretical Contribution
Traditional psychological interventions frequently operate within the content of the client’s cognitive-linguistic history. The Odoki Method inverts this: the backstory is not merely secondary to the process but is actively excluded from it. The pilot data suggest that this exclusion does not impede progress - and may accelerate it, particularly for participants with extensive prior therapeutic experience, for whom narrative engagement may have become its own form of defensive loop.
This is not a claim that narrative is irrelevant to human suffering. It is a more specific claim: that directing attention to the somatic signal prior to its conceptual capture may produce structural change that narrative-level work, however sustained, does not easily reach. This hypothesis is testable, and testing it is a priority for future research.
Reification of the Self-Model: A Proposed Mechanism
The theoretical account developed in this paper proposes that a significant class of psychological suffering is maintained not by specific thoughts or memories but by the structural rigidity of the self-model - the process by which a dynamic biological state becomes organised around the defence of a fixed identity. We have termed this reification of the self-model, and proposed that it represents a common pathway underlying presentations that differ considerably at the level of symptomatic content.
If this account is correct, interventions that address the self-model at the structural level - rather than working on its contents - would be expected to produce broad-spectrum effects across symptom domains. The pattern observed in the WEMWBS data, where improvements in general wellbeing were more consistent than improvements in specific symptom measures, is at least consistent with this prediction. It is not evidence for it.
Limitations
The limitations of this study are significant and should be stated plainly. The sample is small (n=19), recruited entirely through personal networks, and assessed by the same individual who delivered the intervention. There was no control condition, no independent assessment, and no follow-up data. The single-guide design means that observed effects cannot yet be distinguished from individual practitioner skill. Work is underway to address this last point through the training of additional guides, and early indications suggest comparable outcomes, but this has not yet been formally assessed.
Future Research
Before the method can be meaningfully evaluated, the proposed mechanism needs to be more precisely characterised. We propose the following sequence:
Mechanistic studies should be the first priority. The ten-stage sequential structure generates a specific testable prediction: somatic noise should reduce in stepwise fashion across stages three through ten, with each reduction enabling detection of the next target. Identifying appropriate physiological correlates of this remains an open question; heart rate variability is a candidate proxy, though its relationship to the working modality is speculative. Targeted investigations integrating phenomenological data collection at each stage would allow the proposed process of sequential hyperprior destabilisation to be examined directly, rather than inferred from psychometric endpoints alone.
The transdiagnostic framing developed in this paper aligns with patient-identified research priorities for interoception in psychiatry (Hickman et al., 2025), and suggests that mechanistic studies of the Odoki Method may have relevance beyond any single diagnostic category. Phenomenological psychopathology offers the descriptive methodology required to characterise the proposed mechanism at the level of lived experience - a necessary precursor to the computational modelling that could formalise its dynamics.
Expanded cohort studies with independent assessment, a wider recruitment base, and systematic follow-up would strengthen the preliminary psychometric case and provide the data required to specify the population and presentation for which the method is most appropriate.
Randomised controlled trials represent the appropriate endpoint of this research pathway, once the mechanism is sufficiently well characterised to permit the design of a meaningful comparator condition.
The Odoki Method is offered here not as a validated intervention but as a theoretically grounded and empirically promising candidate for systematic investigation. The convergence between the predictive processing account of identity-based suffering, the phenomenological psychopathology literature, and a 2,500-year-old contemplative taxonomy suggests that the structural problem the method addresses is both real and tractable. Whether the method itself is an effective solution to that problem is a question for the research programme outlined above.
References
Barrett, L. F. (2017). The theory of constructed emotion: An active inference account of interoception and categorization. Social Cognitive and Affective Neuroscience, 12(1), 1–23. https://doi.org/10.1093/scan/nsw154
Bodhi, Bhikkhu (trans.). (2012). Saṁyojanasutta (AN 10.13). In The Numerical Discourses of the Buddha: A Translation of the Aṅguttara Nikāya. Wisdom Publications. https://suttacentral.net/an10.13/en/bodhi
Friston, K. (2010). The free-energy principle: A unified brain theory? Nature Reviews Neuroscience, 11(2), 127–138. https://doi.org/10.1038/nrn2787
Gendlin, E. T. (1978). Focusing. Bantam Books. https://archive.org/details/focusing00gendrich
Gendlin, E. T. (1997). Experiencing and the Creation of Meaning: A Philosophical and Psychological Approach to the Subjective. Northwestern University Press. https://nupress.northwestern.edu/9780810114272/experiencing-and-the-creation-of-meaning/
Hickman, L. J., Mackie, G., Longley, B. F., Savage, H. S., Bagley, E., Fleming, H., Knight, R., Lau, I., Whines, A., Garfinkel, S. N., & Nord, C. L. (2025). Breaking through the mind-body divide: patient priorities for interoception research. eClinicalMedicine, 82, 103183. https://doi.org/10.1016/j.eclinm.2025.103183
Laukkonen, R. E., & Slagter, H. A. (2021). From many to (n)one: Meditation and the plasticity of the predictive mind. Neuroscience and Biobehavioral Reviews, 128, 199–217. https://pubmed.ncbi.nlm.nih.gov/34139248/
Laukkonen, R. E., Friston, K., & Chandaria, S. (2025). A beautiful loop: An active inference theory of consciousness. Neuroscience and Biobehavioral Reviews. https://pubmed.ncbi.nlm.nih.gov/40750007/
McParlin, Z., Cerritelli, F., Friston, K. J., & Esteves, J. E. (2022). Therapeutic alliance as active inference: The role of therapeutic touch and synchrony. Frontiers in Psychology, 13, 783694. https://doi.org/10.3389/fpsyg.2022.783694
Metzinger, T. 2003, Being No One: The Self-Model Theory of Subjectivity. MIT Press. https://mitpress.mit.edu/9780262633086/being-no-one/
Sass, L. A., & Parnas, J. (2003). Schizophrenia, consciousness, and the self. Schizophrenia Bulletin, 29(3), 427–444. https://doi.org/10.1093/oxfordjournals.schbul.a007017
Seth, A. K. (2013). Interoceptive inference, emotion, and the embodied self. Trends in Cognitive Sciences, 17(11), 565–573. https://doi.org/10.1016/j.tics.2013.09.007
Seth, A. K., & Tsakiris, M. (2018). Being a beast machine: The somatic basis of selfhood. Trends in Cognitive Sciences, 22(11), 969–981. https://doi.org/10.1016/j.tics.2018.08.008
Stanghellini, G., Broome, M., Fernandez, A. V., Fusar-Poli, P., Raballo, A., & Rosfort, R. (Eds.). (2019). The Oxford Handbook of Phenomenological Psychopathology. Oxford University Press. https://academic.oup.com/edited-volume/27976
Thompson, E. (2007). Mind in Life: Biology, Phenomenology, and the Sciences of Mind. Harvard University Press. https://www.hup.harvard.edu/books/9780674057517